Authors
- Dr. Rawshan Zahan Akhter Alo, Principal Investigator and Deputy Director, Institute of Public Health Nutrition, Ministry of Health and Family Welfare
- Dr. Ashek Mahfuz, Portfolio Lead, LSFF and Value Chain, Bangladesh, GAIN
- Md. Abul Bashar Chowdhury, Project Manager, Large Scale Food Fortification, Bangladesh, GAIN
Micronutrient deficiencies, particularly those of vitamin D and Folate, are global public health concerns that significantly affect populations in developing regions. Vitamin D deficiency affects over one billion people globally, with 37.3% having serum levels below 50 nmol/L, particularly in sun-limited regions and high-risk populations [1–4]. In South Asia, over 70% of women and children are deficient [5, 6]. In Bangladesh, data from National Micronutrient Survey 2019-20, revealed vitamin D deficiency among under-five children (22.60%) and NPNL mothers (70.60%), which indicates major population-level evidence gaps.
The clinical consequences of Vitamin-D deficiency extend beyond bone diseases such as rickets, osteomalacia, and osteoporosis. Vitamin D has been implicated in several non- skeletal conditions, including cardiovascular diseases, diabetes, autoimmune diseases, and certain cancers [7]. Deficiency has also been associated with poor immune response, increasing susceptibility to infections, including respiratory tract infections and COVID- 19.
Assessment on Prevalence of Vitamin D deficiency
To get a more comprehensive understanding of the wide range of Vitamin D and Folate deficiency in Bangladesh, GAIN and the Institute of Public Health Nutrition (IPHN) conducted an assessment on “Prevalence of Vitamin D and Folate Deficiency among People of Different Age Groups in Bangladesh”. The study was conducted from January to July 2025, with a total of 2481 individuals from five age groups (children, adolescents, pregnant women, adults, and geriatric individuals) people blood samples analysed for Serum Vitamin D (25-hydroxyvitamin D) and Serum Folate levels collected from eight divisions of Bangladesh, covering urban and rural areas.
Figure 1: Overall Vitamin D Status (n=2480) Figure 2: Vitamin D Status in Urban and Rural
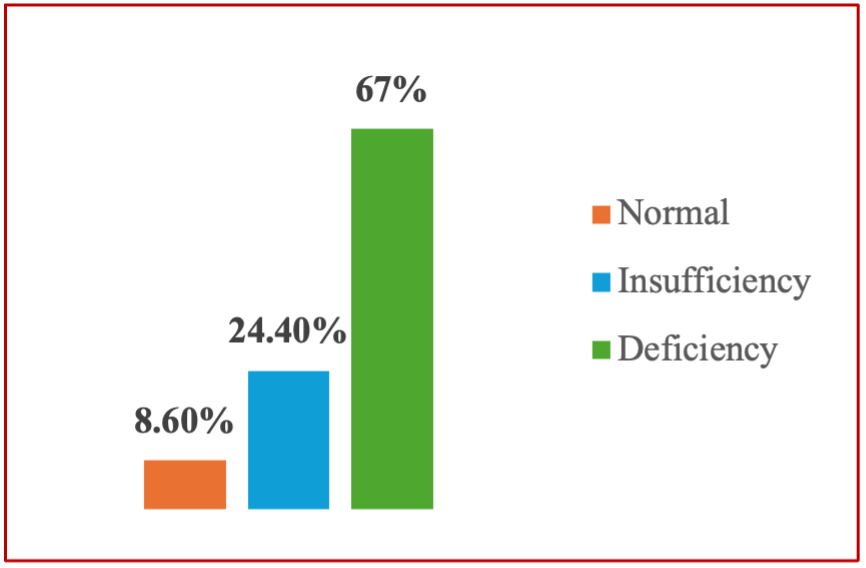
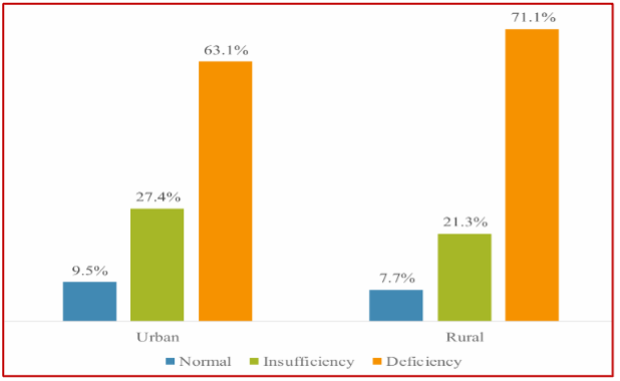
The results of the study revealed a significant 67.0% of participants to be deficient in vitamin D. The deficiency rates were highest among adolescents (83.3%) and pregnant women (77.8%). Urban residents (71.1%) exhibited higher deficiency rates compared to rural residents (63.1%).
This national survey highlights vitamin D deficiency as a major public health concern affecting all age groups in Bangladesh, with adolescents, pregnant women, and females most at risk. Clear geographic disparities exist, particularly in the southeastern and southern regions. These findings show that micronutrient gaps, especially vitamin D remain inadequately addressed due to the lack of national fortification policies and uneven access to supplements. Without timely and targeted interventions, long-term consequences may include poor bone and immune health, pregnancy complications and cognitive decline across the population.In Bangladesh, GAIN is implementing the Digitizing Fortification Quality and Strengthening Enabling Environment project in partnership with the regulatory agencies, refineries, academia, and development partners, under the leadership of the Ministry of Industries.
As part of this initiative, GAIN supports the amendment of fortified edible oil standards to include both vitamin A and vitamin D. Currently, edible oil in Bangladesh is fortified only with vitamin A. The inclusion of vitamin D aims to address the high prevalence of vitamin D deficiency in the country and improve overall public health outcomes.
Conclusion:
Vitamin D deficiency remains a critical public health issue across all age groups, especially among adolescents, pregnant women, and females. The findings underscore the need for comprehensive public health interventions, including food fortification programs. In Bangladesh, fortification of edible oil with Vitamin A is mandatory. Now the edible oil fortification standard and laws can be amended and fortified with vitamin A and D to alleviate the deficiencies of these two vital micronutrients to all segments of the population in Bangladesh.
References:
1. Palacios C, Gonzalez L. Is vitamin D deficiency a major global public health problem? J Steroid Biochem Mol Biol. 2014;144 Pt A:138-45.
2. Cashman KD, Dowling KG, Škrabáková Z, et al. Vitamin D deficiency in Europe: pandemic? Am J Clin Nutr. 2016;103(4):1033-44.
3.Forrest KYZ, Stuhldreher WL. Prevalence and correlates of vitamin D deficiency in US adults. Nutr Res. 2011;31(1):48-54.
4.Hilger J, Friedel A, Herr R, et al. A systematic review of vitamin D status in populations worldwide. Br J Nutr. 2014;111(1):23-45.
5.Islam MZ, Lamberg-Allardt C, Kärkkäinen M, et al. Vitamin D deficiency in Bangladesh: a study in pregnant women. Eur J Clin Nutr. 2002;56(1):51-6.
6. Harinarayan CV, Joshi SR. Vitamin D status in India—its implications and remedial measures. J Assoc Physicians India. 2009;57:40-8.
7. Holick MF. Vitamin D status: measurement, interpretation, and clinical application. Ann Epidemiol. 2009;19(2):73-8.
8. Martineau AR, Jolliffe DA, Hooper RL, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ. 2017;356:i6583.
9. Panfili FM, Roversi M, D'Argenio P, et al. Possible role of vitamin D in Covid-19 infection in pediatric population. J Endocrinol Invest. 2021;44(1):27-35.